SSA-3368 EDCS Screenshots (Revised for PRW NPRM)
Intermediate Improvement to the Disability Adjudication Process: Including How We Consider Past Work - RIN 0960-AI83
SSA-3368 EDCS Screenshots (Revised for PRW NPRM)
OMB: 0960-0834
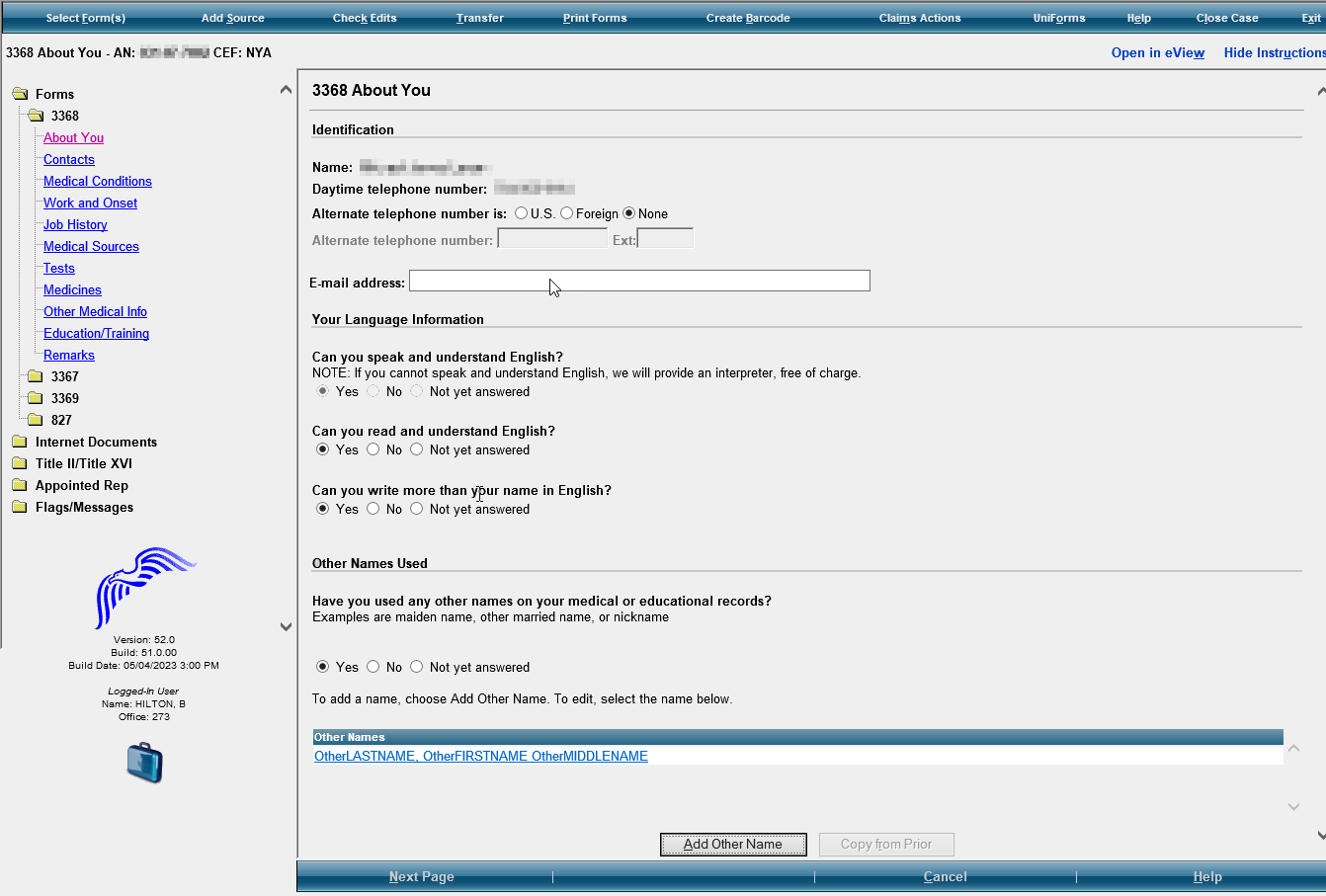
SSA-3368 EDCS Screenshots for PRW NPRM
About You/ Section 1- Information About You
Modify
the examples to read as follows: “Examples
include
maiden name, other married names, other
names,
or nickname.”
Modify
to read: “Daytime numbers where we can call to speak with you
or leave a message, if needed.” Add
“Primary” to add the number Modify
Alternate to “Secondary”
Include-
Suffix for the name
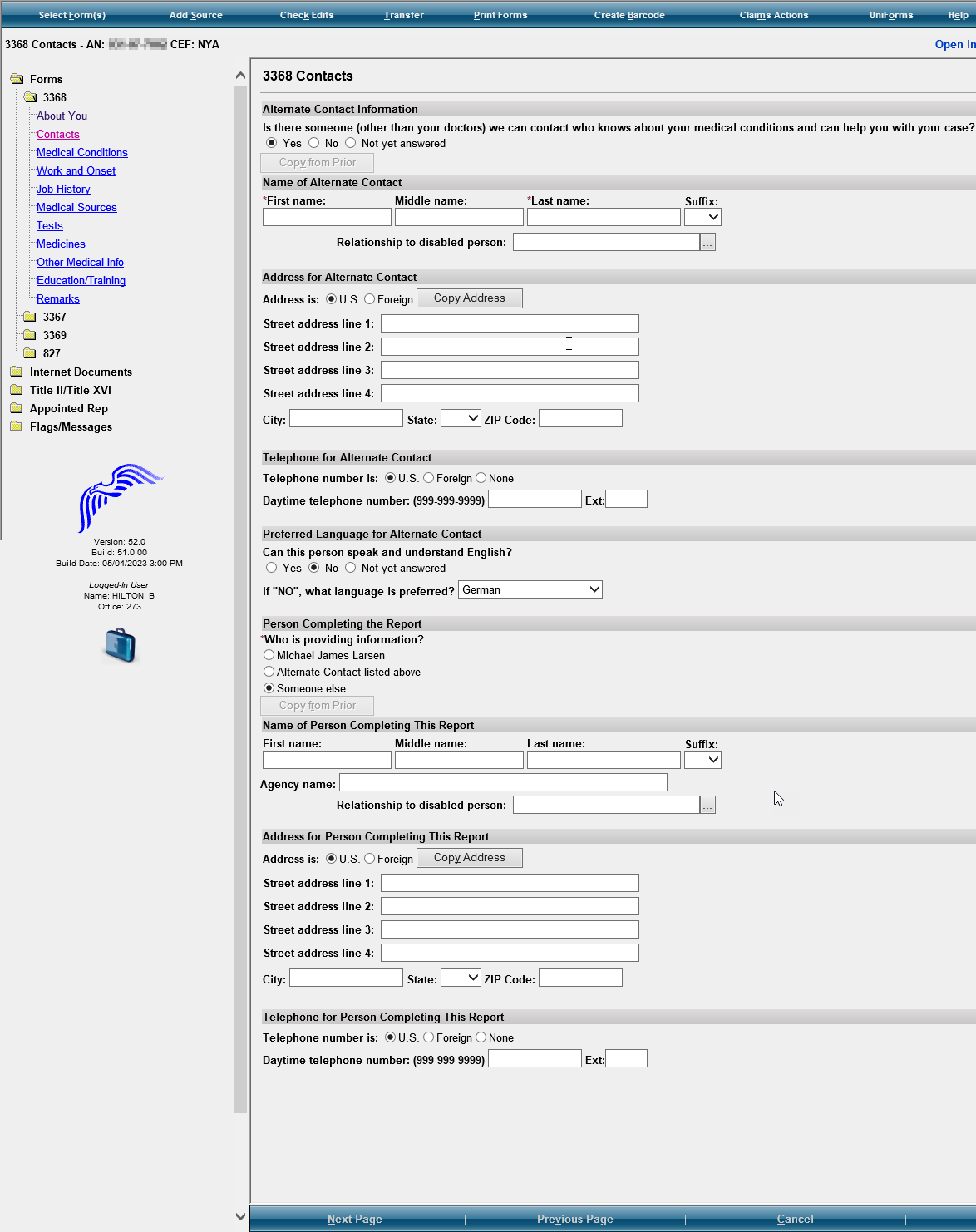
3368 Contacts/ Section 2- Contacts

In the 3368 Contacts section, modify section subtitles to the following:
Alternate Contact title to “Contact Person Information”
Name of Alternate Contact title to “Name of Contact”
Address for Alternate Contact to “Address for Contact”
Telephone for Alternate Contact to “Telephone for Contact”
Preferred Language for Alternate Contact to “Preferred Language of Contact”
When adding a second contact, the subtitles should be “Additional Contact Person”
Please move the Person Completing the Report Section, Name of Person Completing this Report, Address for Person Completing the Report, and Telephone for Person Completing the Report to the end of the screens after the Remarks screen.
Modify
the question to read as follows: “Is
there someone we can contact who can help with your claim if needed?
Examples include a family member, friend, or neighbor.” Add
the ability to enter two contacts. “Contact
Person Information” and “Additional Contact Person
Information” If
they select yes, add: “Please provide the names of two people
(other than your doctors) we can contact who know about your medical
condition(s) and can help you with your claim and can help us reach
you if you become unavailable.” If
they select no, add: “We recommend that you provide at least
one contact, if available. Providing the name of someone who knows
you may help us to make a quicker decision on your claim.” Add
section to provide an additional contact with Name, Relationship to
You, Address of the person, Daytime phone number of this person, and
Preferred Language.
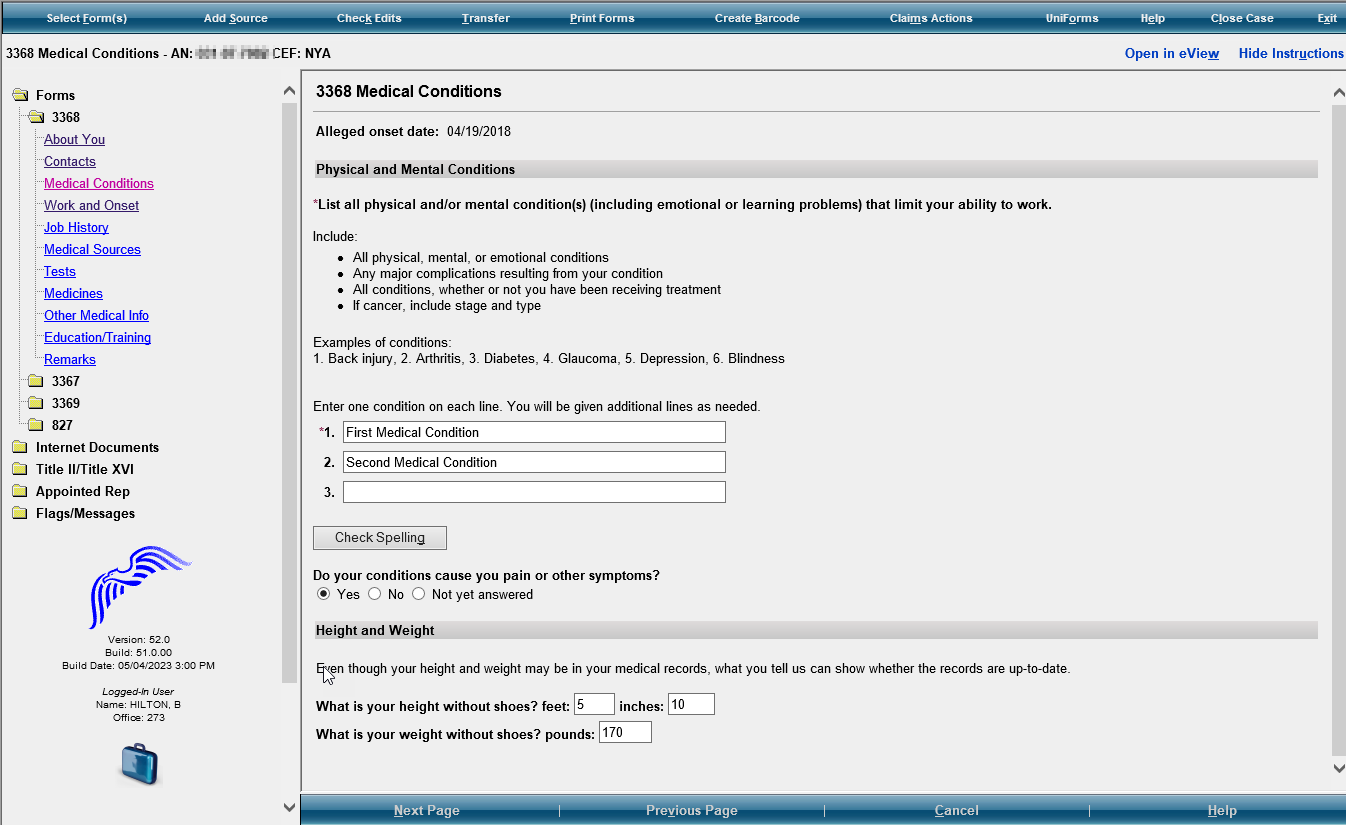
Medical Conditions/ Section 3- Medical Information


In the Height and Weight section remove the instructions that say, “Even though your height and weight may be in your medical records, what you tell us can show whether the records are up to date”. No instructions needed.
Modify the Height and Weight questions to read as follows:
“What is your height?” Add text and radio box to include “OR centimeters”
“What is your weight?” Add text and radio buttons to include “OR kilograms”
Remove this question.
Modify the instructions to read as follows:
“Separately list each physical and/or mental condition that limits your ability to work.”
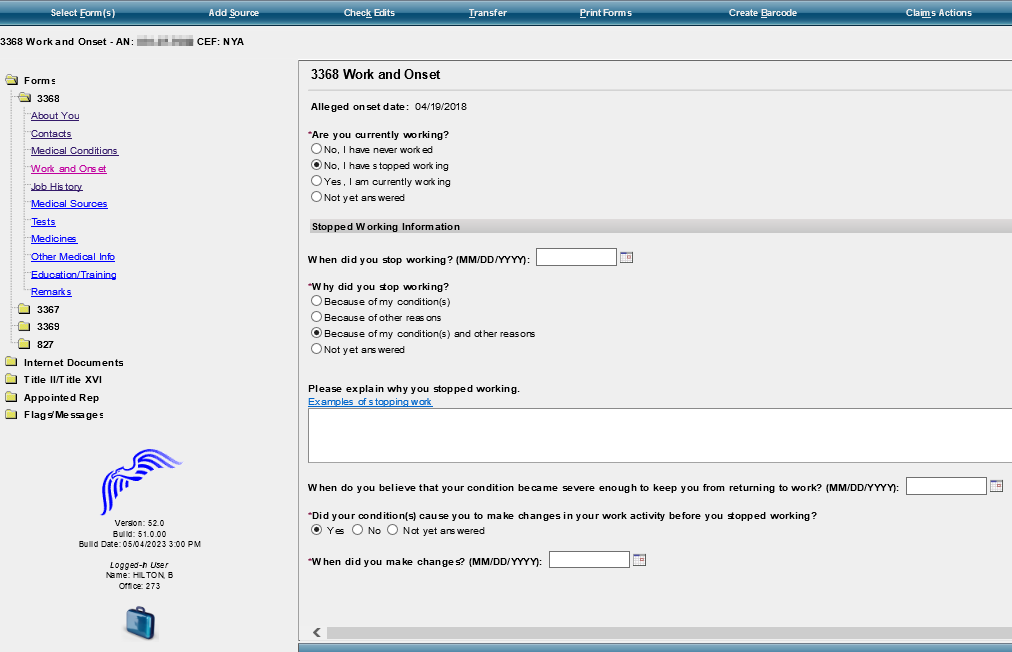
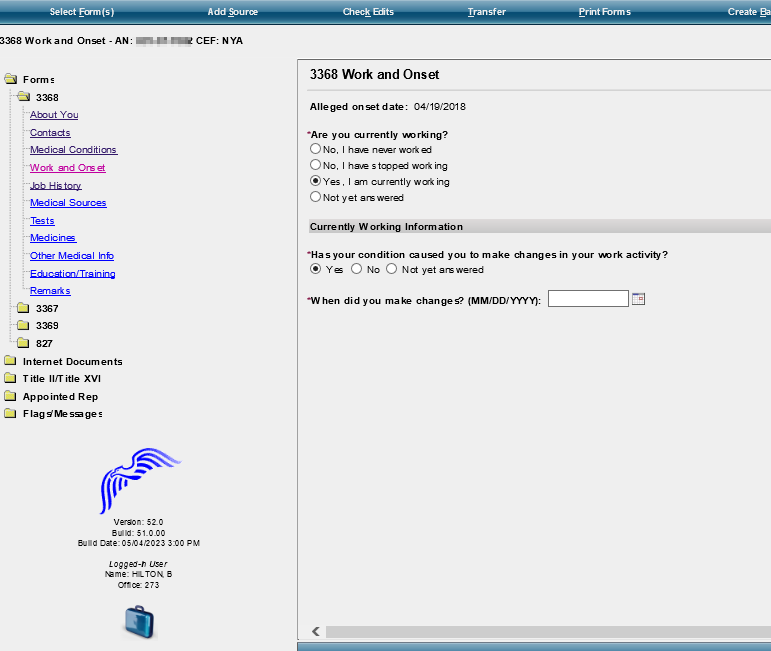
Work and Onset/ Section 4- Work Activity
With answer “No, I have stopped working”
Modify the last radio button option “Because of other reasons” to say:
“Because of other reasons. Please explain the other reasons why they stopped working. Examples include laid off, early retirement, seasonal work ended, or business closed.”
Modify
the question to read as follows: “Did your condition(s) cause
you or
your employer to
make changes in your work activity? Examples
include job duties, hours, or rate of pay.”
If
yes, modify the question to read as follows: “When
did the changes start?”
MM/DD/YYYY format
With Answer “Yes, I am currently working”
Modify
the question in the to read as follows: “Has
your condition(s)
caused you
or
your employer to
make changes in your work activity? Examples
include job duties, hours, or rate of pay.” If
yes, modify question to read,
“When did the changes start?” If
no, modify the question to read,
“When did your condition(s) first start bothering you?”
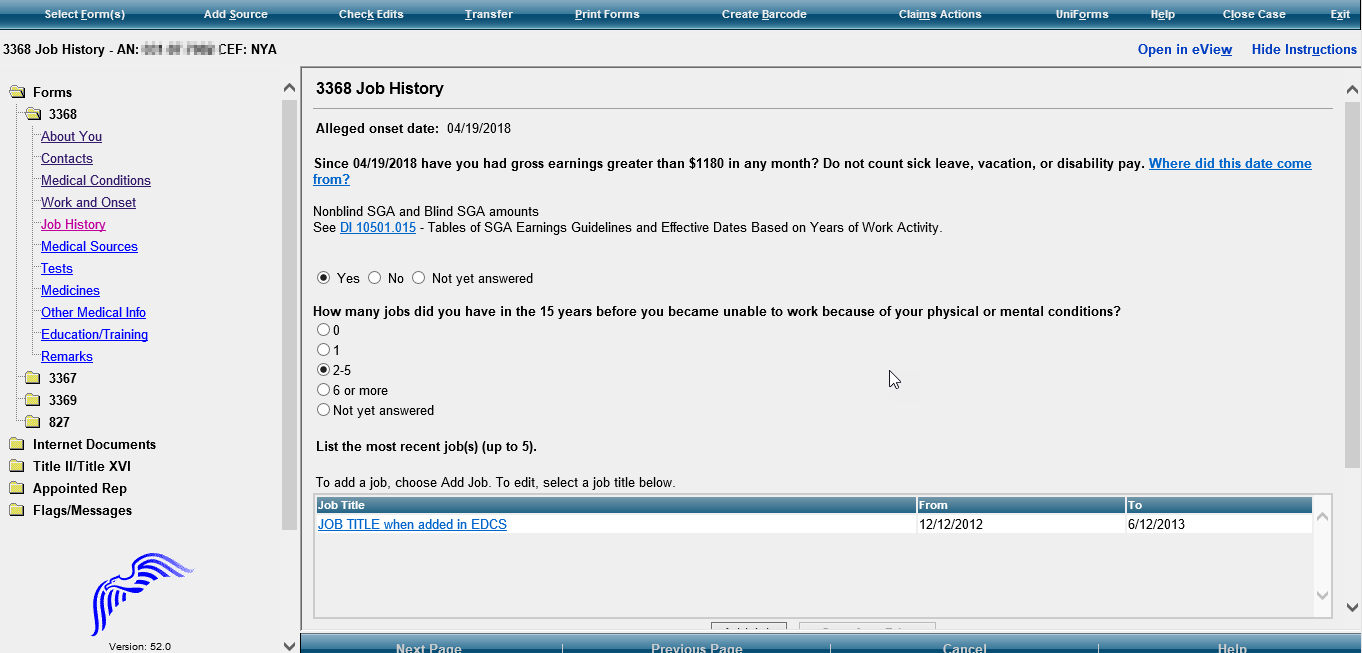
Job History/ Section 6- Work History


Modify
the instructions to say: “List the jobs (up to 5) that you had
in the past 5 years. List all
the jobs that you have had in the last 5
years: Include
self-employment Include
work in a foreign country List
your most recent job first”
Add question: “Did
you have a job in the last 5 years?” Add
checkboxes to select YES NO
If yes,
modify Job Listing instructions to say, “Select
the number of jobs you have had in the past 5 years”.
Modify
this question to read:
“Since
….have you had earnings greater than $____before
tax
in any month?”
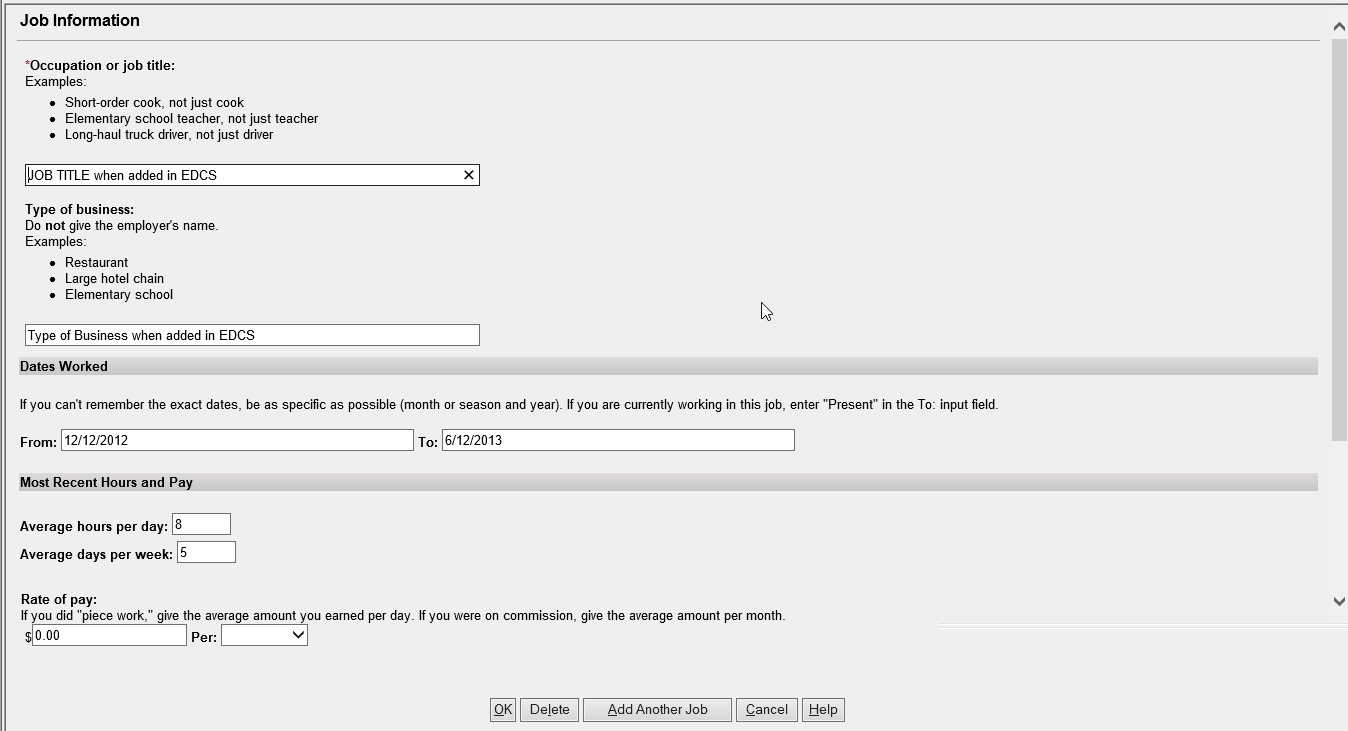
Job Information Page

For Rate of Pay- Frequency in drop-down should be Per: hour, day, week, month, or year
Section 6.B- Information about your work
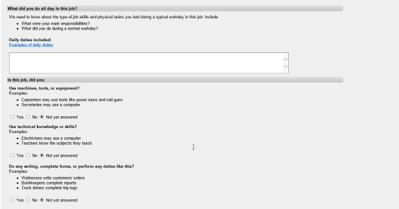
Modify
the questions to read as follows: “For
this job, describe in detail the tasks that you did in a typical
workday. Examples of tasks include stocking shelves, greeting
customers, scheduling appointments, and maintaining records.”
Add
a text box for description. “If
any tasks listed above involved writing or completing reports,
describe the type of report that you wrote or completed and how much
time you spent on it per workday or workweek.” Add
a text box for description. If
any of the tasks listed above involved supervising others, describe
who and what you supervised and what supervisory duties you had.
Examples of supervisory duties include performance management,
making schedules, or maintaining time records.” Add
a text box for explanation. “List
the machines, tools, and equipment you used regularly when doing
this job and explain what you used them for. Examples of equipment
include computer, telephone, forklift, air compressor, and meat
slicer.” Add
a text box for description. “Tell
us about the work-related skills you used in this job. Examples of
work-related skills include reading blueprints to instruct workers
on how to build houses and medical coding to determine the amounts
providers should be paid.” Add
a text box for explanation. Add
this question, “Did
your job require you to interact with coworkers, the general public,
or anyone else?”
If
they select yes, add the following instructions: “Describe
who you interacted with, the purpose of this interaction, how you
interacted, and how much time you spent doing it per workday or
workweek. Examples include answering customer questions on the
telephone for 5 hours per day or showing clients sale properties for
4 hours per day.” Add
a text box for explanation.
![]() YES
YES
![]() NO
NO
Section 6C. Physical requirements of your work
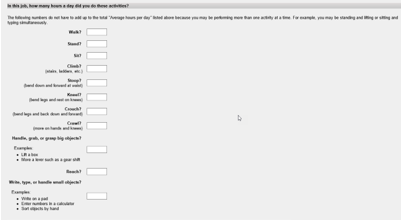
Modify
the instructions to read: “Tell
us how much time you spent performing the following physical
activities in a typical workday. The total hours/minutes for
standing and/or walking and sitting should equal the Hours per Day.
The
example below shows an 8-hour workday with 2 hours standing and/or
walking and 6 hours sitting (8 hours total).” For
each activity, add text boxes for “Hours/Minutes” to
indicate activity identify activity times.
* The
paper form includes an “Example” text box that shows how
many hours/minutes for each activity. Standing and walking- 2 hours;
stooping- 6 minutes. Work with Systems to determine how to include
this on EDCS.
Combine
walk and stand to show,
“Standing and/or Walking”
Sit to
“Sitting”
Modify the activity section accordingly:


Stoop to
“Stooping”;
keep explanation

Kneel to “Kneeling”; keep explanation
Crouch
to “Crouching”;
keep explanation
Crawl to
“Crawling”;
keep explanation
Using
fingers to touch, pick, or pinch (e.g., using a mouse, keyboard,
turning pages, or buttoning a shirt)
Add radio buttons to select One Hand and Both Hands
Using
hands to seize, hold, grasp, or turn (e.g., holding a large
envelope, a small box, a hammer, or water bottle);
Add radio buttons to select One Hand and Both Hands
Reach to
“Reaching
at or below the shoulder”;
Add radio button to select One Arm and Both Arms

Reaching overhead (above the shoulder): Add radio buttons to select One Arm and Both Arms
Climb
to “Climbing stairs or ramps”
“Climbing
ladders, ropes, or scaffolds”

Modify the question to “Select the weight frequently lifted (i.e., 1/3 to 2/3 of the workday)”. Add “Less than 1 lb.” to the list of options in the drop down.
Modify
the question to “Select
the heaviest weight lifted”
Add “Less
than 1 lb.”
to the list of options in the drop down.
Modify
Physical Activities Lifting and Carrying instructions: “Tell
us about lifting and carrying in this job. Explain what you lifted,
how far you carried it, and how often you did it in a typical
workday.”

After
last heaviest weight question, add this question: “Did
your job expose you to any of the following? Check all that apply.”
Add radio buttons and text to select the following options:
“ Outdoors
If
one or more of the options are checked, add a text box with
instructions that say, “Tell
us about the exposure(s) and how often you were exposed.”
![]() Extreme Heat (non-weather related)
Extreme Heat (non-weather related)
![]() Extreme Cold (non-weather related)
Extreme Cold (non-weather related)
![]() Wetness
Wetness
![]() Humidity
Humidity
![]() Hazardous Substances
Hazardous Substances
![]() Moving Mechanical Parts
Moving Mechanical Parts
![]() High
Exposed Places
High
Exposed Places
![]() Heavy Vibration
Heavy Vibration
![]() Loud Noise
Loud Noise
![]() Other”
Other”

Remove the two questions “Did you supervise other people in this job?” and “Were you a lead worker.
Add this question and a textbox for explanation:
“Explain how your medical conditions affect your ability to do this job.”

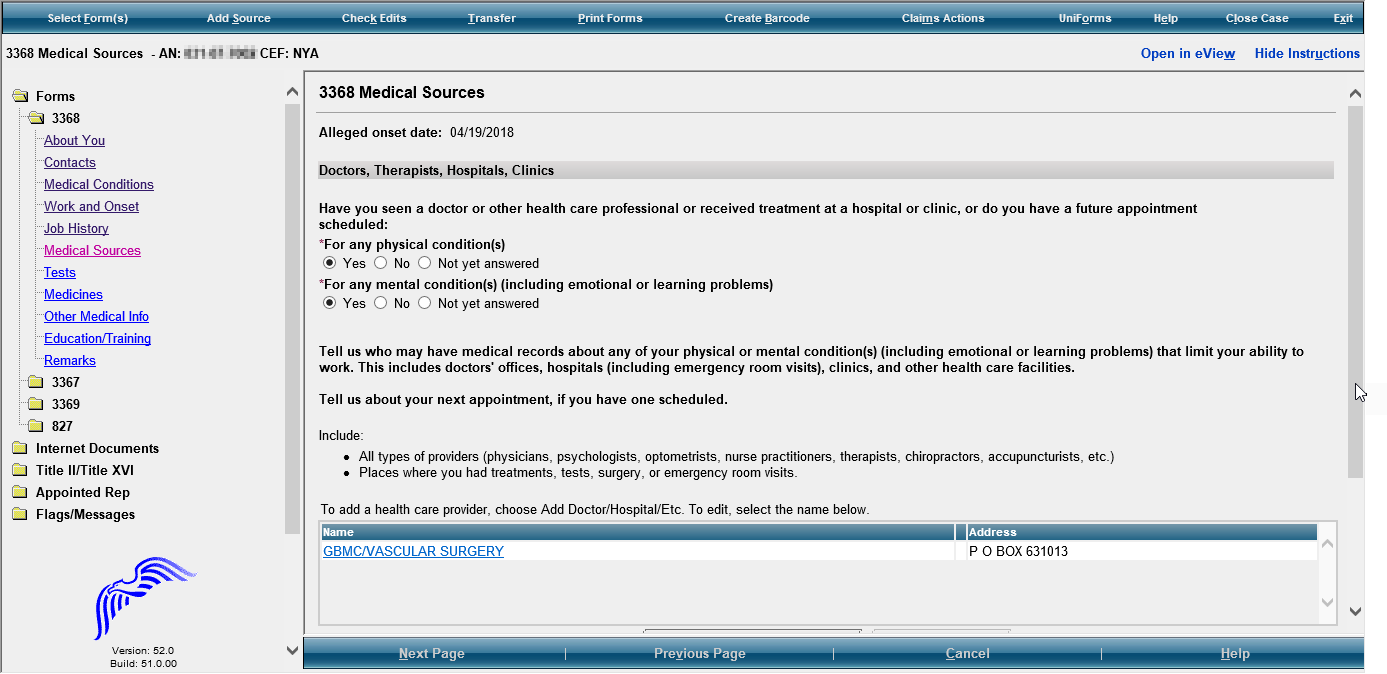
Medical Sources/ Section 8- Medical Treatment

Modify section title to read “Medical Treatment”
Modify this question to read, “Have you seen or received treatment from a health care provider (doctor, hospital, clinic, psychiatrist, nurse practitioner, therapist, physical therapist, or other medical professional) or do you have a future appointment scheduled?
Add, “You may find this information on medical bills, online medical chart, or the internet.”
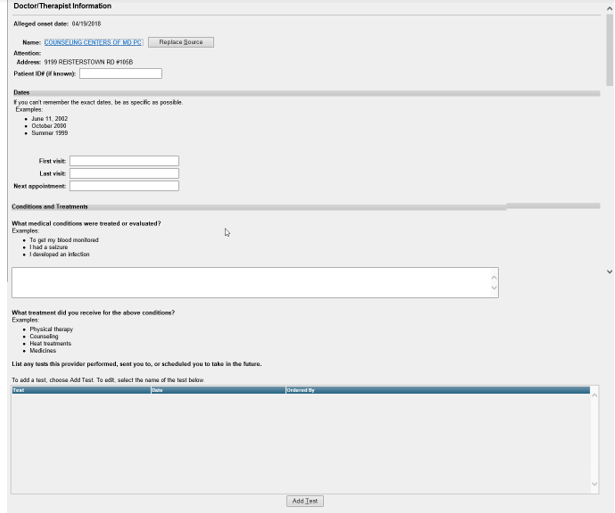
Doctor/Therapist Information

Modify as follows
“Name of Facility or Office”
“Name of Healthcare Provider that treated you”
“Phone Number”
“Street Address”
“City”
“STATE/Province”
“ZIP/Postal Code”
Remove Patient ID # (if known)
In Dates section, modify the Dates boxes as follows:
“Date First Seen: MM/YYYY”
“Date Last Seen: MM/YYYY”
“Date Next Seen: MM/YYYY”
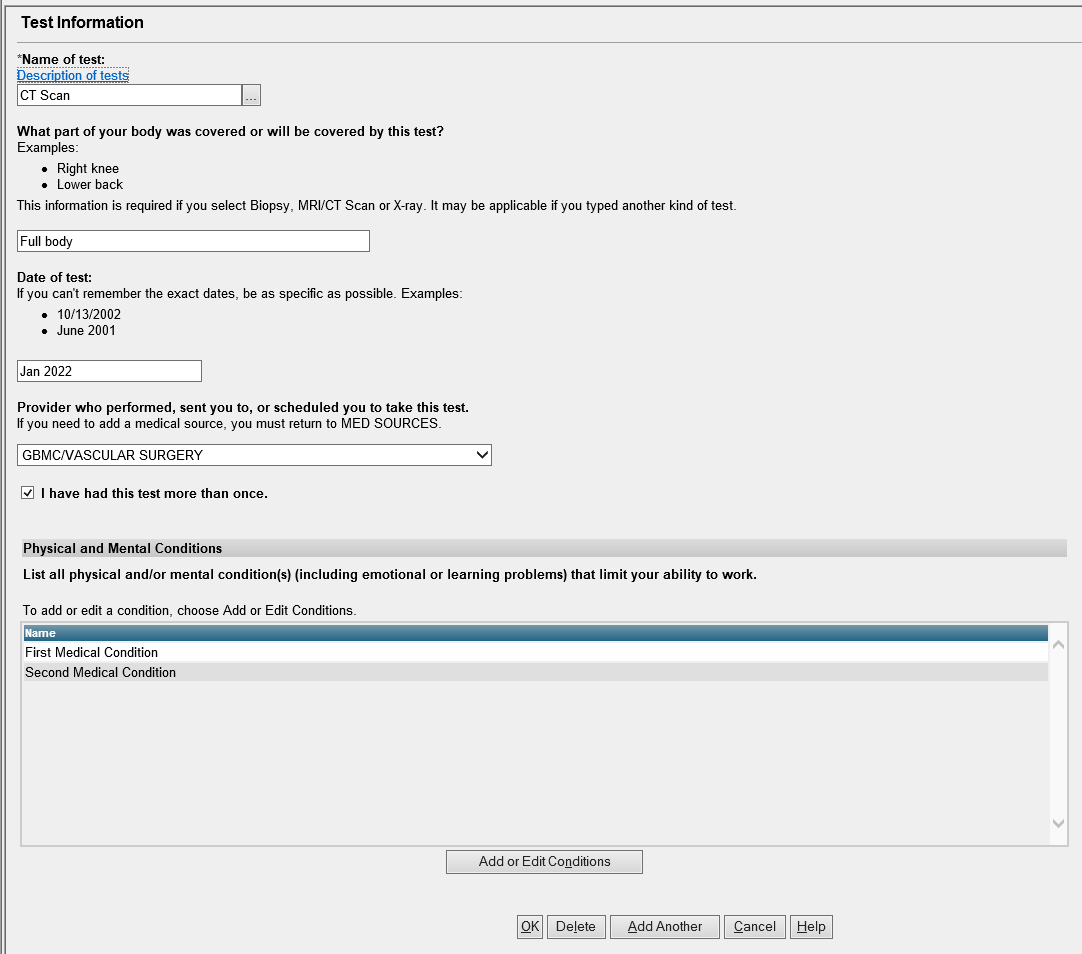
Tests/ Section 8B- Medical tests
Modify this question read, “Did any of the providers order any medical tests for you? Include tests already performed and scheduled in the future.”
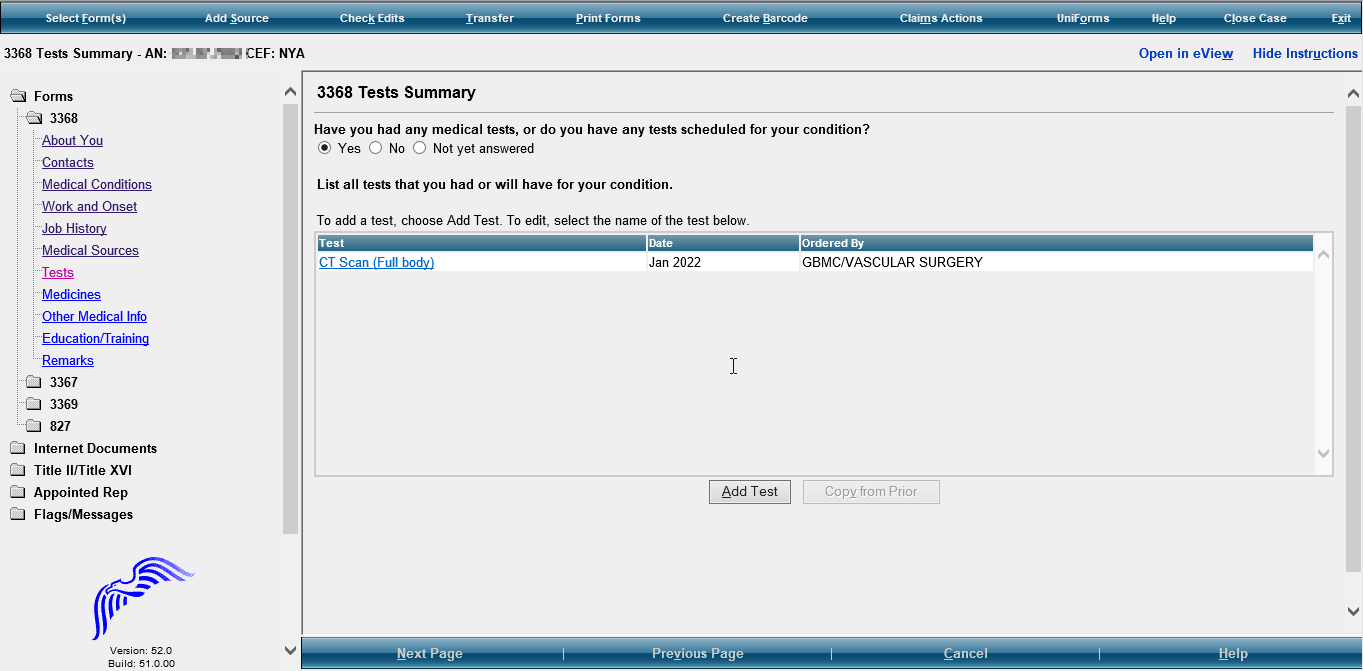
Test Information
Modify
instructions, “Provider who performed, sent you to, or
scheduled you to take this test” to “Name
of healthcare provider or facility
who performed, sent you to, or scheduled you to take this test.”
Add
“Psychological/IQ
test”
to drop down selection to “Name of test” If
“Other”, add “please
specify” and provide a text box for explanation. Date
of test should be in MM/YYYY format
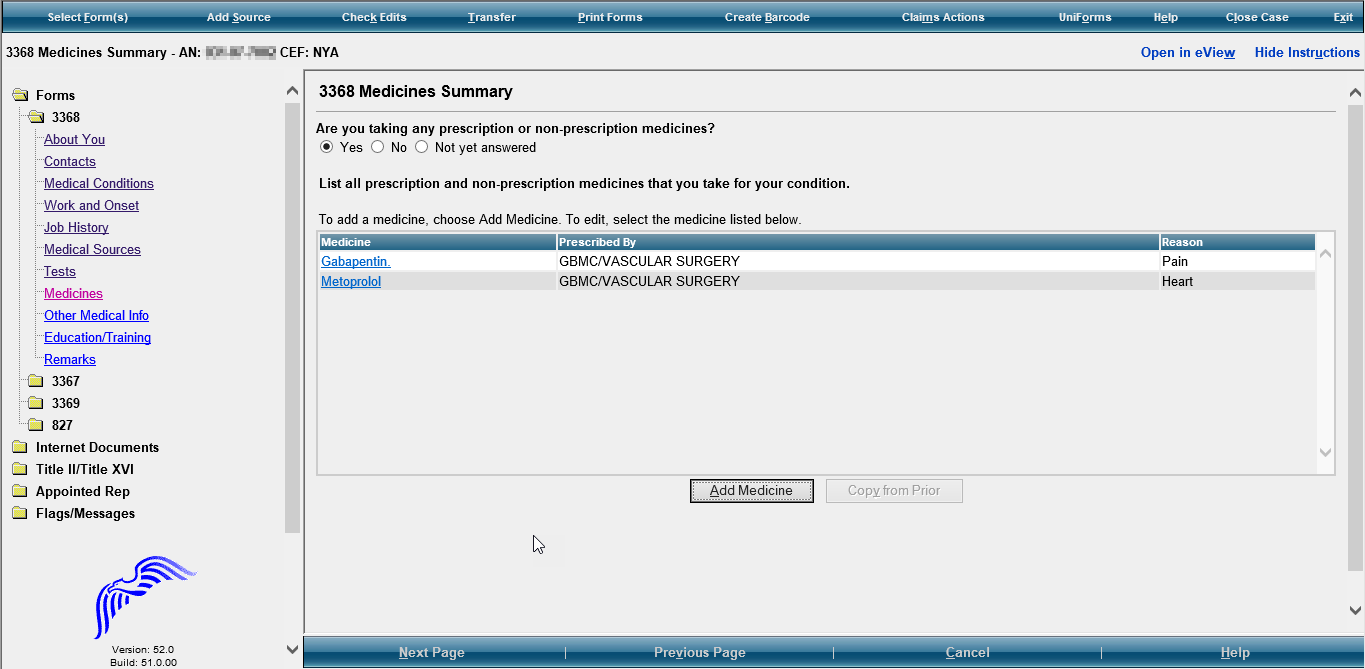
Medicines/ Section 7- Medicines
Modify instructions in listing medication section:
Prescribed By- “If Prescribed Give Doctor Name (If Known)”
Reason- “Reason for Medicine (If Known)”
Modify this question to read, “Are you currently taking any prescription or non-prescription medicine(s)?”
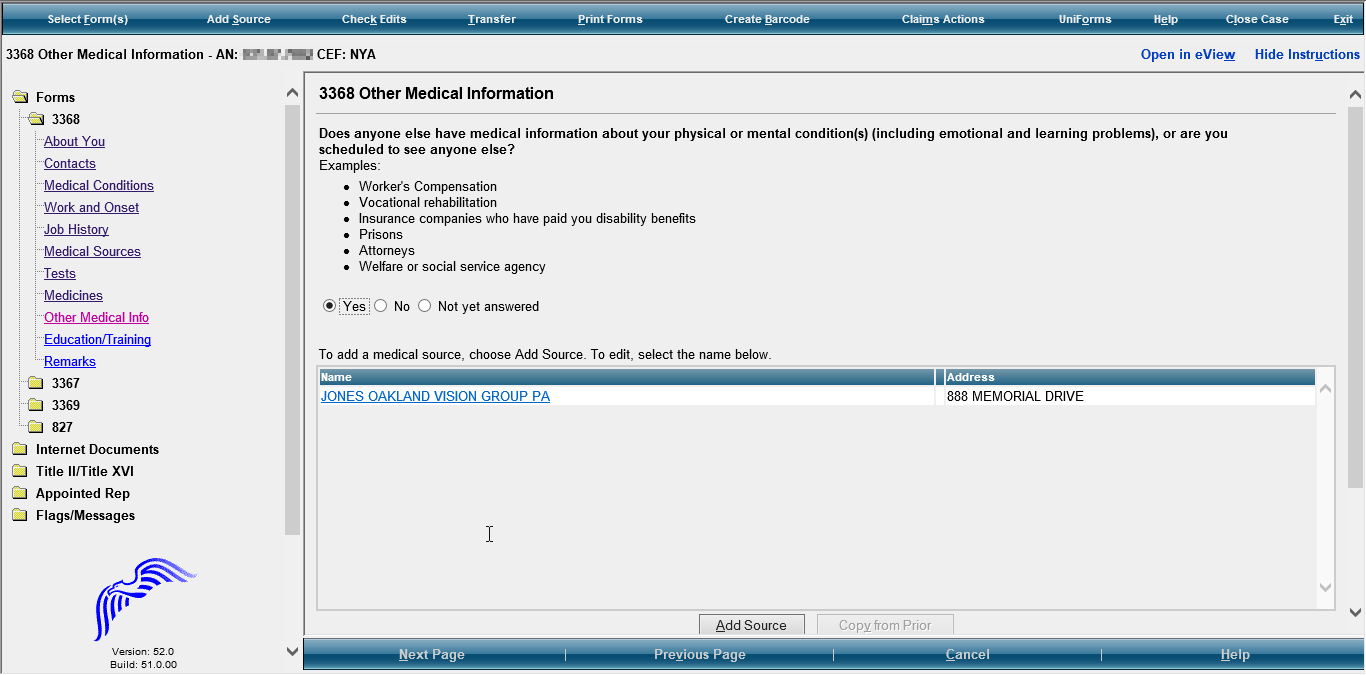
Other Medical Info/ Section 9- Other Medical Information
If yes, provide text boxes for:
“Name or Organization, Phone Number, Mailing Address, City, State/Province, Zip/Postal Code, Country (if not USA), Name of Contact Person, Claim Number (if any), Date of First Contact, Date of Last Contact, Date of Next Contact (if any), Reason(s) for Contacts”
Modify this question to read, “Does anyone else (other than your medical providers) have your medical information? Examples include social service agencies, welfare agencies, attorneys, prisons, workers’ compensation, and insurance companies who have paid you disability benefits.”

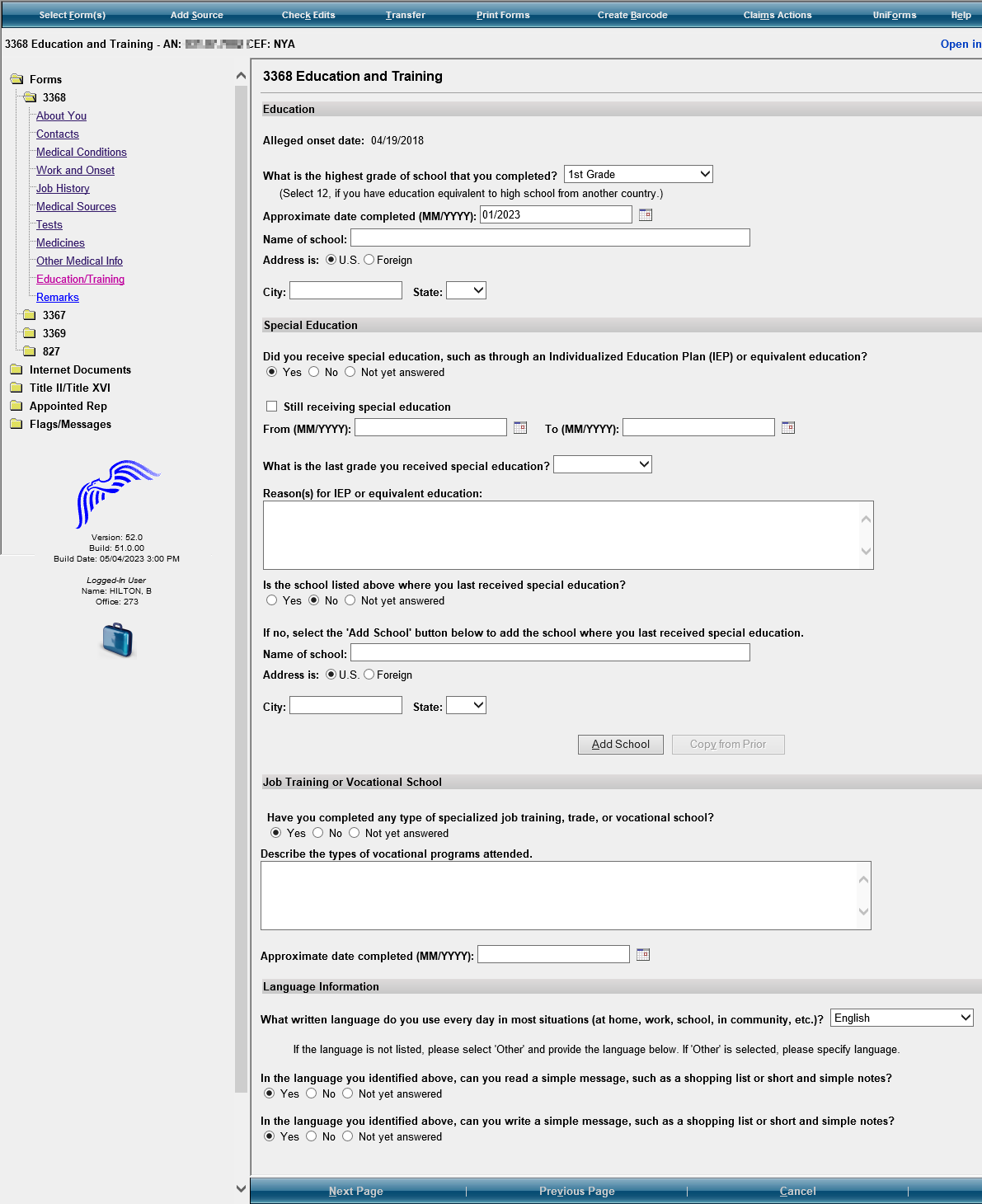
Modify Education and Training Section title to: “Education, Training and Literacy”
Education and Training






Modify this question to read, “If no, select the ‘Add School’ button below to add the school where you were last in special education.”
Modify this question to read, “Is the school listed above where you were last in special education?”
In Job Training or Vocational School, modify question to read, “Have you received any type of training (specialized job trade, or vocation training)?” Text box instructions should say “Type of Program”
Modify question: Did you receive special education, such as through an IEP…) to “Were you in special education?”
Modify Reason(s) for IEP or equivalent education to: “Reason(s) for special education:”
Modify section title to “Literacy Information”
Modify
the first question to read, “Select
the highest level of high school completed, including
homeschooling, online education, and education received in another
country. Select “12” if you completed a graduate
equivalence degree (GED).” Keep
the drop down box to select the highest grade of school completed
from the drop down selections. Add
“College 1, 2, 3, 4”
to the drop-down selections.
Modify
the question to read, “Select
the last grade you were in special education.”
In
Language Information, modify the questions to read, “READING-
In the language you identified…can you read…? WRITING-
In the language you identified… can you write…?”
If yes,
add sections to complete: “Name
of Training Facility, Phone Number, Mailing Address, City,
State/Province, Zip/Postal Code, Country (if not USA), Type of
Program, Date Completed (or scheduled to be completed)”
MM/YYYY format. Keep text box for Type of Program

Modify this question to read, “Have you completed any type of training (specialized job, trade, or vocational training)?
If yes, special education was received, modify this question to read, “Select the last grade you received special education.”
Modify
these two questions to read,
“READING-
In the language that you identified above can you read...?” “WRITING-
In the language you identified above can you write….?”
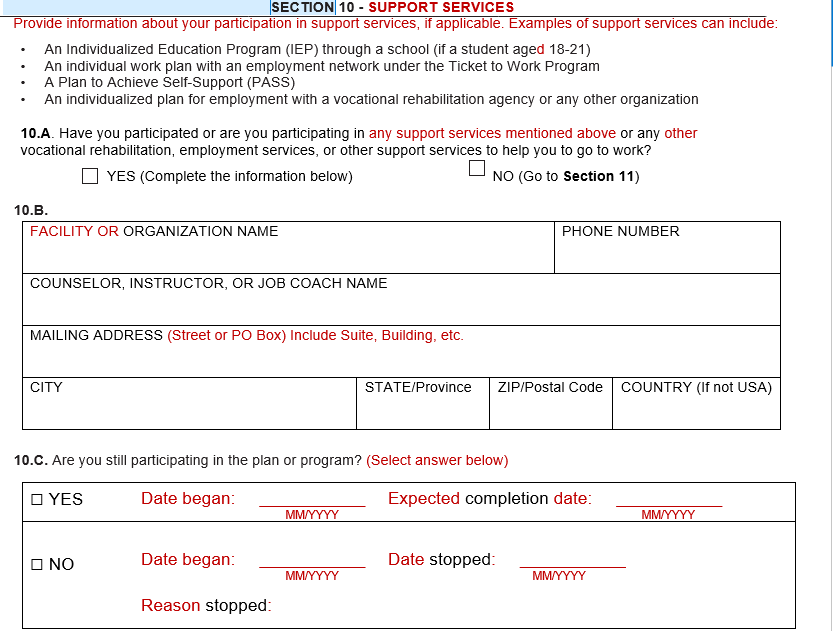
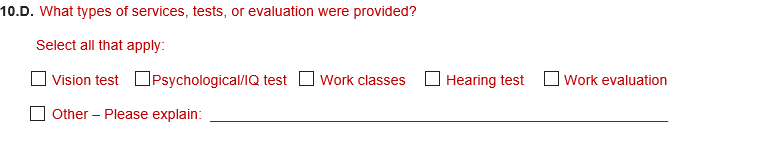
Support Services
Please add this section/page at the end of the Education and Training Section (before REMARKS).
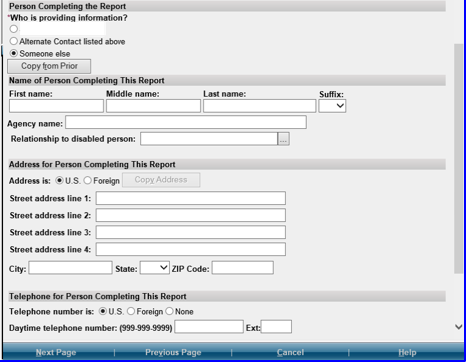
Section 11- Remarks Section- Here
Modify
this section as follows: Remove
Who is providing the information? Add
the following” “Date
Report Completed (MM/DD/YYYY)” “Who
is completing this report?” Add
radio buttons and the following options: “John
Doe Contact
Person Additional
Contact Person Someone
else If
they select radio button for Someone else, provide text boxes to
complete the following information: Name
(First, Middle Initial, Last) Relationship
to John Doe Mailing
Address (Street or PO Box) include the apartment number, if
applicable. CITY STATE/Province ZIP/Postal
Code Country
(if not USA) DAYTIME
PHONE NUMBER where we may reach you or leave a message, if needed.
Include the area code or IDD and country code if outside the USA or
Canada.” 
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Modified | 0000-00-00 |
| File Created | 0000-00-00 |
© 2025 OMB.report | Privacy Policy